SHOT Show is the largest trade show of its kind covering shooting sports, outdoor, hunting and law enforcement industries. Stay tuned for live coverage coming from Day 3 of SHOT Show 2016!
This post will update throughout the day as our coverage continues, so check back often for all the awesomeness! All new content will be posted at the top so there’s no need to scroll down, simply keep refreshing the page to view posts as we send them in.

–1830– Leaving well after dark on another full day from SHOT Show 2016. Coverage continues tomorrow, same bat time, same bat channel.



–1531– Checking out Triumph Systems and their innovative new target solutions. Their Pivotal Trainer is a mobile turning target system retailing for $399. Their Pop Packs and Threat Down Responsive Targets showcase proper shot placement with hi-vis gels. ^BB



–1412– Darley Defense Rescue Task Force concept kit, comes with two vests, helmets, gloves, and eye pro. It also comes with a medical bag full of re-supply items. ^ES

–1400– Tactical Electronics K9 camera kit, remote viewing from the K9 perspective. ^ES

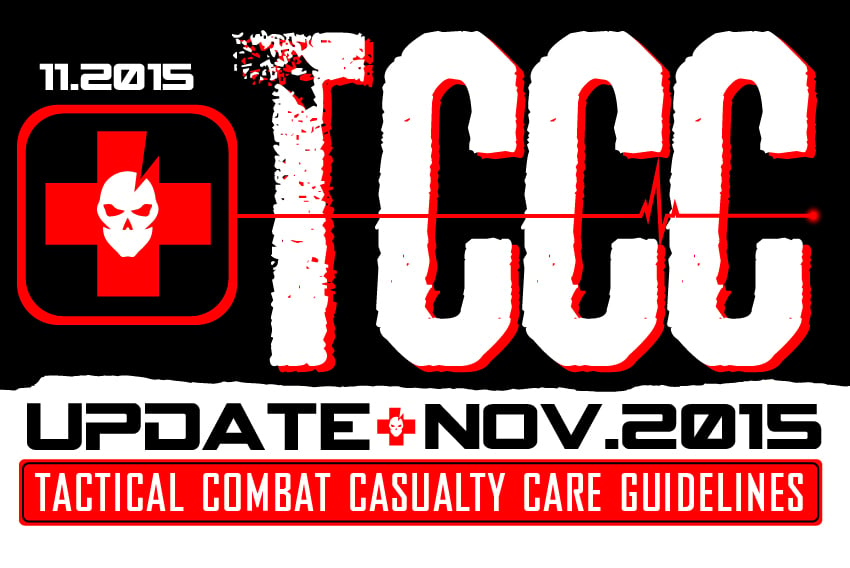
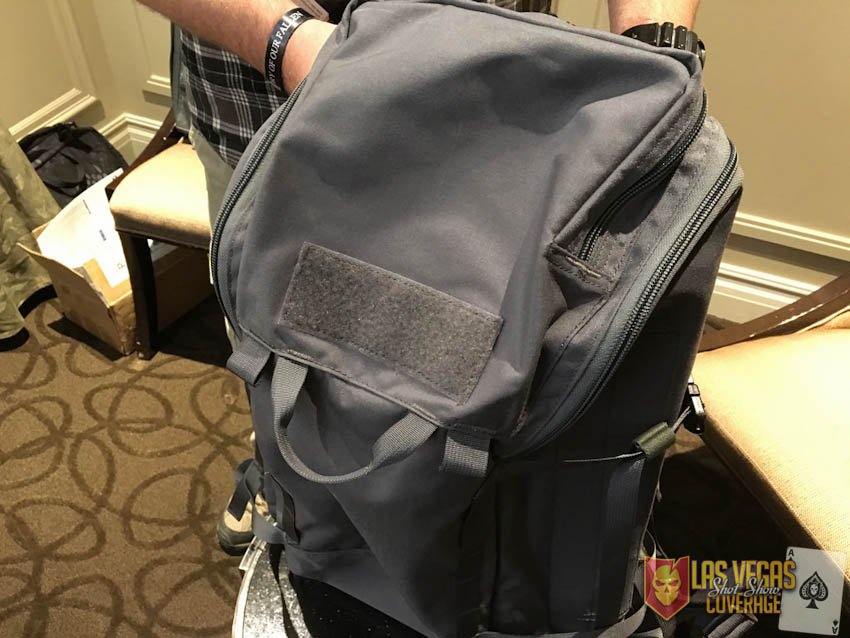
–1359– Mystery Ranch’s Overload pack, with rifle carry functionality. ^MNS

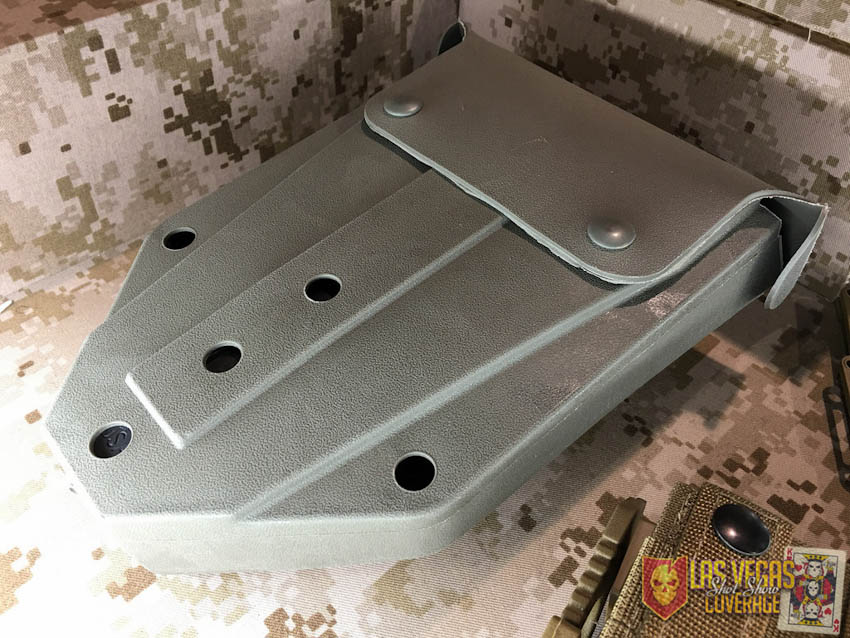
–1358– Mystery Ranch RATS medical bag, interesting design which filets open. ^ES

–1317– Agency Arms race guns on parade. ^MNS

–1316– Agency Arms wing suit at their booth. ^MNS



–1313– JJFU’s suppressor in cutaway is on display, as well as a new bolt gun and 300WM semi-auto rifle. ^MNS



–1304– Mystery Ranch’s wide line of packs. ^MNS

–1220– Point Blank’s 4025 Elite Bomb Suit. ^MNS

–1215– Barrett has an M240-LW on display. ^MNS

–1213– Emerson Knives have a new knife made for Sig Sauer for their Legion product line. ^MNS

–1208– A close view of Gore’s Advanced Combat Fabric on view at the Gore booth. ^MNS



–1205– Beyond Clothing and Outdoor Research are experimenting with Gore’s Topo material, both on display at the Gore booth. ^MNS

–1204– Wild Things insulated MultiCam jacket in new Gore material called GORPYRAT. ^MNS

–1157– For the Butterfly fans out there. The blades in these are pretty trick. ^ES

–1156– Some of the many AXIS lock knives, these have been going strong for 15 years. ^ES
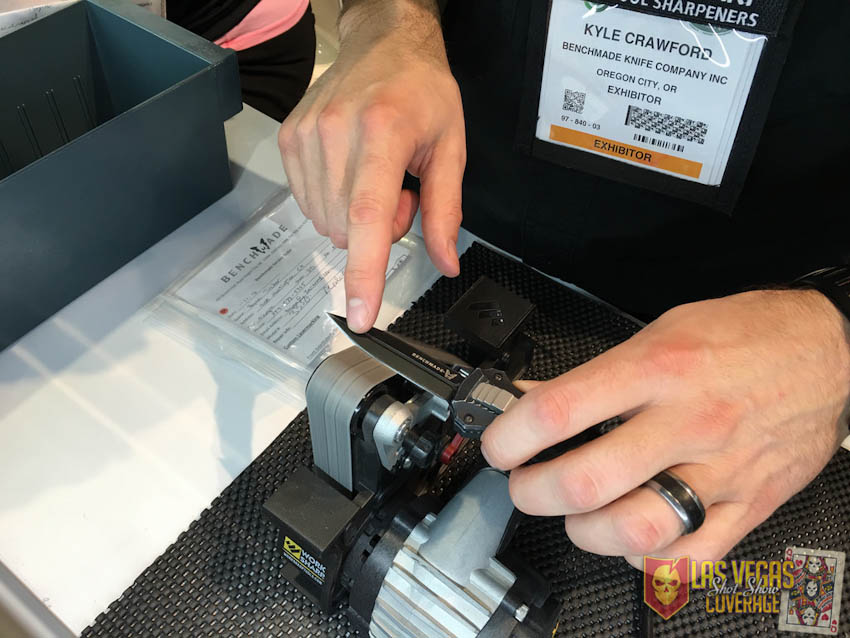
–1153– Bring your Benchmade knife by for a full cleaning, sharpening, and laser engraving all at once. ^ES


–1145– Glock G17 MOS configuration, with pre-milled slide and four plates allowing for a wide variety of optic mounting. ^MNS

–1144– Glock 17 Gen 4 9mm. ^MNS

–1143– Neat cutout display of a G17 Gen4. ^ES

–1142– These are picking up speed at my agency with the guys doing plain clothes work. ^ES


–1141– Glock’s single stack 9mm G43, in a hand for size reference. ^MNS

–1139– SIGs line of suppressors, there are a lot of companies breaking into the “shush gun” market. ^ES


–1139– I carried a standard 226 in the Army, but this Enhanced Elite with laser device would have been much better. ^ES

–1137– Sig’s Romeo4 compact red dot sight. ^MNS


–1133– Sig Sauer’s Legion 220 and Full Size RX P320 ^MNS


–1130– Do you think red dot sights, lights, and lasers will be common place on pistols in the near future? Could be. ^ES


–1129– Some of SIGs LEO offerings. ^ES

–1128– Pretty basic, but this is what I trust my life and the lives of my partners on at work. ^ES

–1127– Colt M-240B and M-240L. ^MNS

–1126– Colt Gatling gun anyone? ^ES

–1125– Colt M4 OWM1, ready for customization. ^MNS

–1123– The Military Commemorative Rifle and Pistol program. You can have 2 lines of text on both sides of the slide, custom graphics, unit logo and custom serial number. ^ES

–1122– Colt’s M4 Magpul Edition rifles. ^MNS

–1120– Colt’s IAR6940 infantry automatic rifle. ^MNS

–1115– Remote control system at the Colt booth, pretty neat. ^ES

–1000– Just finished up recording a new episode of Gear Tasting, so look forward to that coming out soon! Live coverage will resume in just a bit from the floor of SHOT Show 2016!

–0757– Had an amazing mobility workout this morning, learning from Scott Sonnon of TACFIT Academy. Pictured on the left is Sayoc Kali guru Harley Elmore, who I also look forward to training with more. ~ Bryan
Looking for more coverage?
You can also follow along through Twitter, Facebook, Instagram and Google+.
Don’t forget that all orders placed in the ITS Store during the week of SHOT Show will get a free limited edition ITS Casino Plaque! Offer ends 1/22/16 11:59 EST, while supplies last.